·
What
is Cardiotocography?
Cardiotocography:(CTG) is used in pregnancy to
monitor both the fetal heart as well as the contractions of the uterus. It is
usually only used in the 3rd trimester. Its purpose is to monitor fetal
well-being & allow early detection of fetal distress. An abnormal CTG
indicates the need for more invasive investigations & ultimately may lead
to emergency caesarian section.
How it
works
The
device used in cardiotocography is known as a cardiotocograph.It involves the
placement of 2 transducers on the abdomen of pregnant women. One transducer
records the fetal heart rate using ultrasound. The other transducer monitors
the contractions of the uterus. It does this by measuring the tension of the
maternal abdominal wall. This provides an indirect indication of intrauterine pressure.
The CTG is then assessed by the midwife & obstetric medical team.
How to
read a CTG
To
interpret a CTG you need a structured method of assessing its
variouscharacteristics. The most popular structure cans be rememberedusing the
acronym DR C BRAVADO
DR – Define Risk
C – Contractions
BRa – Baseline Rate
V – Variability
A –
Accelerations
D – Decelerations
O - Overall impression
O - Overall impression
Define
risk
You
first need to assess if this pregnancy is high or low riskThis isimportant as
it gives more context to the CTG reading
E.g. If the pregnancy is high risk, your threshold for
intervening may be lowered
Reasons a pregnancy may be
considered high risk are shown below¹
Maternal medical illness
Gestational diabetes
Hypertension
Asthma
Hypertension
Asthma
Obstetric complications
Multiple gestation
Post-date gestation
Previous cesarean section
Intrauterine growth restriction
Premature rupture of the membranes
Congenital malformations
Oxytocin induction/augmentation of labor
Pre-eclampsia
Post-date gestation
Previous cesarean section
Intrauterine growth restriction
Premature rupture of the membranes
Congenital malformations
Oxytocin induction/augmentation of labor
Pre-eclampsia
Other risk factors
No prenatal care
Smoking
Smoking
Drug abuse
Contractions
Record
the number of contractions present in a 10 minute period - e.g. 3
in 10
Each
big square is equal to 1 minute, so you look how manycontractions occurred in
10 squares
Individual
contractions are seen as peaks on the part of the CTG monitoring uterine
activity
You
should assess contractions for the following:
§ Duration – how long do the contractions last?
§ Intensity – how strong are the contractions? (assessed
using palpation)
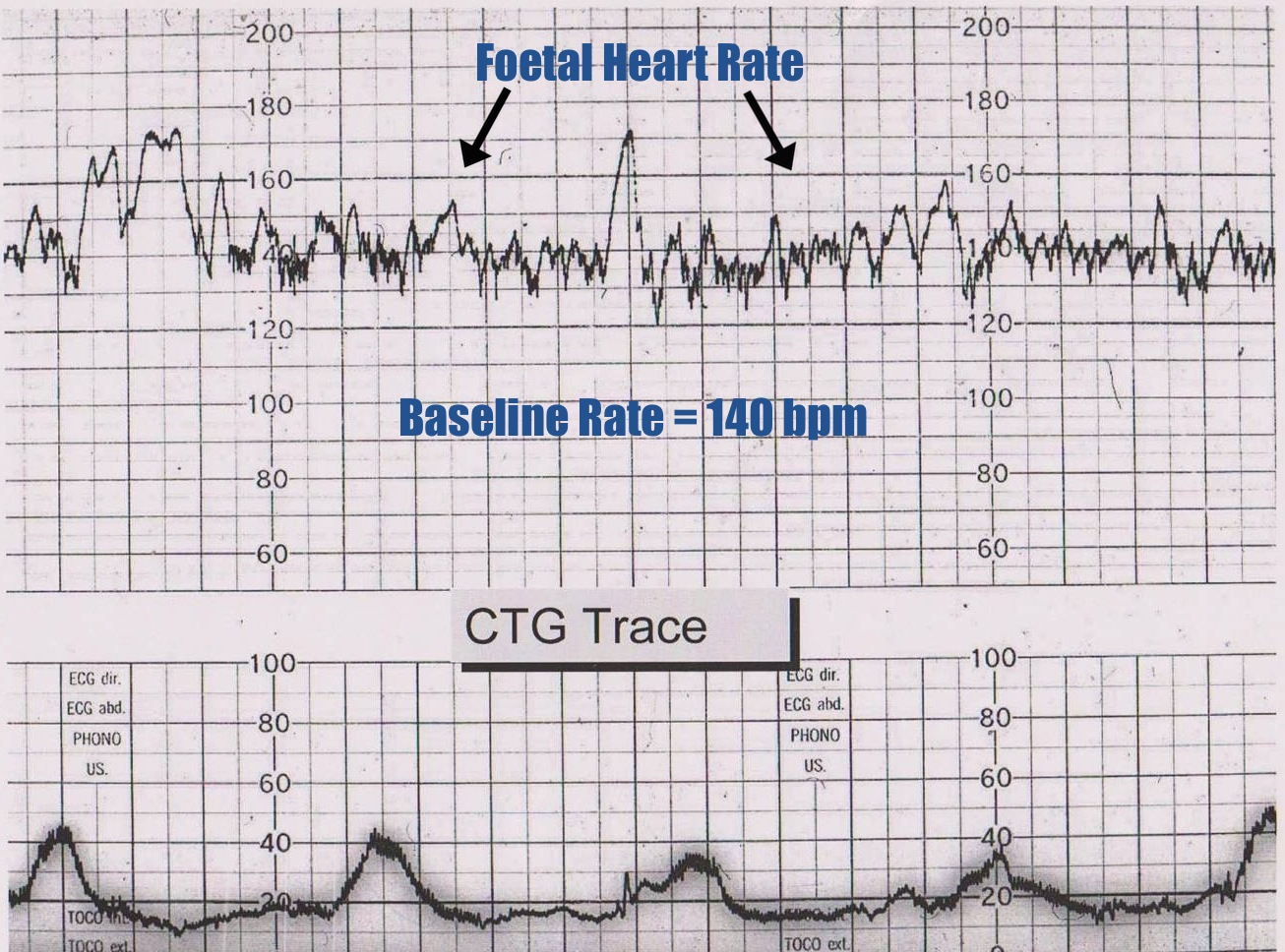
In this example there are 2-3
contractions in a 10 minute period - e.g. 3 in 10
..
Baseline
rate of fetal heart
The baseline rate is the average
heart rate of the fetus in a 10 minute window
Look at the CTG & assess what
the average heart rate has been over the last 10 minutes
Ignore any Accelerations or
Decelerations
A normal fetal heart rate is between
110-150 bpm¹
{kind=link}
Fetal Tachycardia
Fetal
tachycardia is defined as a baseline heart rate greater than 160 bpm
It
can be caused by:
§ Fetal hypoxia
§ Chorioamnionitis – if
maternal fever also present
§ Hyperthyroidism
§ Fetal or Maternal Anemia
§ Fetal tachyarrhythmia
Fetal Bradycardia
Fetal
bradycardia is defined as a baseline heart rate less than 120 bpm.
Mild
bradycardia of between 100-120bpm is common in the following situations:
§ Post-date gestation
§ Occiput posterior or transverse
presentations
Severe
prolonged bradycardia (< 80 bpm for > 3 minutes) indicates severe hypoxia
Causes of prolonged severe
bradycardia are:
§ Prolonged cord compression
§ Cord prolapse
§ Epidural & Spinal Anesthesia
§ Maternal seizures
§ Rapid fetal descent
If
the cause cannot be identified and corrected, immediate delivery is recommended
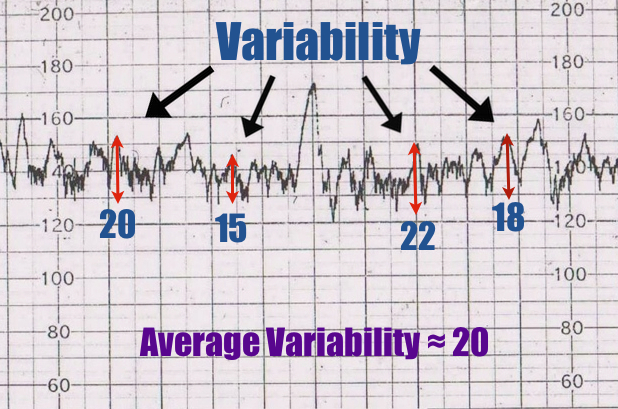
Variability
Baseline
variability refers to the variation of fetal heart rate from one beat to the
nextVariability occurs as a result of the interaction between the nervous
system, chemoreceptors, baroreceptors& cardiac responsiveness. Therefore it
is a good indicator of how healthy the fetus is at that moment in time. This is
because a healthy fetus will constantly be adapting it’s heart rate to respond
to changes in its environment.
.
Normal variability is between 10-25
bpm³
To calculate variability you look at
how much the peaks & troughs of the heart rate deviate from the baseline
rate (in bpm)
.
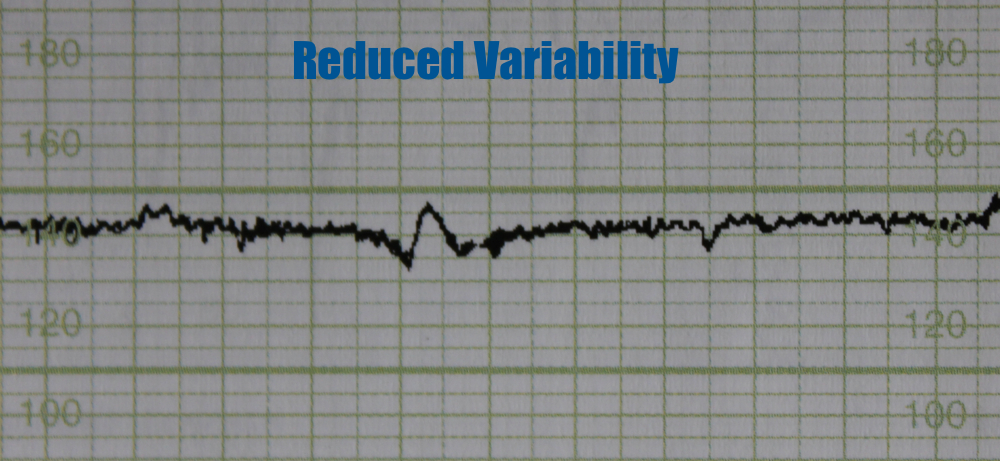
Variability can be categorized
as:
§ Reassuring – ≥ 5 bpm
§ Non-reassuring – < 5bpm for
between 40-90 minutes
§ Abnormal – < 5bpm for >90
minutes
{kind=link}
..
Reduced variability can be caused
by:
§ Fetus sleeping - this should
last no longer than 40 minutes – most common cause
§ Fetal acidosis (due to hypoxia)
– more likely if late decelerations also present
§ Fetal tachycardia
§ Drugs – opiates, benzodiazepine’s,
methyldopa, magnesium sulphate
§ Prematurity – variability is
reduced at earlier gestation (<28 weeks)
§ Congenital heart abnormalities
{kind=link}
.
Accelerations
Accelerations
are an abrupt increase in baseline heart rate of >15 bpm for >15 seconds
The
presence of accelerations is reassuring
Antenatal
there should be at least 2 accelerations every 15 minutes¹
Accelerations
occurring alongside uterine contractions is a sign of a healthy fetus
However
the absence of accelerations with an otherwise normal CTG is of uncertain
significance
{kind=link}
Decelerations
are an abrupt decrease in baseline heart rate of >15 bpm for >15 seconds
There
are a number of different types of decelerations, each with varying
significance
.
Early
deceleration
Early
decelerations start when uterine contraction begins & recover when uterine
contraction stops
This
is due to increased fetal intracranial pressure causing increased vagal tone
It
therefore quickly resolves once the uterine contraction ends & intracranial
pressure reduces
This
type of deceleration is therefore considered to be physiological & not
pathological
{kind=link}
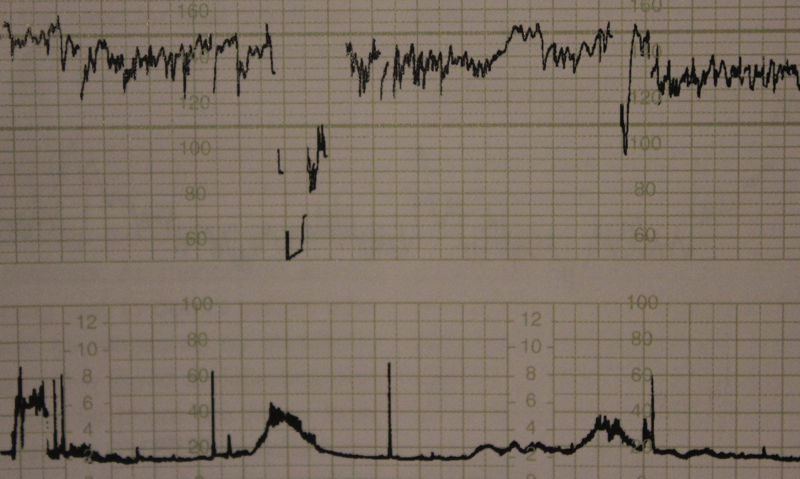
Variable
deceleration
Variable
decelerations are seen as a rapid fall in baseline rate with a variable
recovery phase
They
are variable in their duration & may not have any relationship to uterine
contractions
They
are most often seen during labor& in patients with reduced amniotic fluid
volume
Variable
decelerations are usually caused by umbilical cord compression
§ The umbilical vein is often occluded
first causing an acceleration in response
§ Then the umbilical artery is
occluded causing a subsequent rapid deceleration
§ When pressure on the cord is reduced
another acceleration occurs & then the baseline rate returns
§ Accelerations before & after a
variable deceleration are known as the “shoulders of deceleration”
§ There presence indicates the fetus
is not yet hypoxic & is adapting to the reduced blood flow.
Variable
decelerations can sometimes resolve if the mother changes position
The
presence of persistent variable decelerations indicates the need for close
monitoring
Variable
decelerations without the shoulders is more worrying as it suggests the fetus
is hypoxic
{kind=link}
.
Late deceleration
Late
decelerations begin at the peak of uterine contraction & recover after the
contraction ends.
This
type of deceleration indicates there is insufficient blood flow through the
uterus & placenta
As
a result blood flow to the fetus is significantly reduced causing fetal hypoxia
& acidosis
.
Reduced utero-placental blood flow
can be caused by:
§ Maternal hypotension
§ Pre-eclampsia
§ Uterine hyper-stimulation
.
The presence of late decelerations
is taken seriously &fetal blood sampling for pH is indicated
If fetal blood pH is acidotic it
indicates significant fetal hypoxia & the need for emergency C-section
{kind=link}
…
Prolonged deceleration
A
deceleration that last more than 2 minutes
If
it lasts between 2-3 minutes it is classed as Non-Reassuring
If
it lasts longer than 3 minutes it is immediately classed as Abnormal
Action
must be taken quickly – e.g. fetal blood sampling / emergency C-section
.
Sinusoidal
Pattern
This
type of pattern is rare, however if present it is very seriousIt is associated
with high rates of fetal morbidity & mortality
.
It is described as:
§ A smooth, regular, wave-like pattern
§ Frequency of around 2-5 cycles a
minute
§ Stable baseline rate around 120-160
bpm
§ No beat to beat variability
A sinusoidal pattern indicates:
§ Severe fetal hypoxia
§ Severe fetalanemia
§ Fetal/Maternal Hemorrhage
.
Immediate C-section is indicated for this kind of
pattern.Outcome is usually poor
.
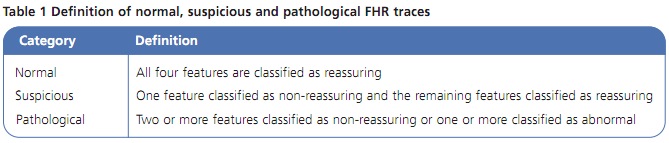
Overall
impression
Once
you have assessed all aspects of the CTG you need to give your overall
impression
The
overall impression can be described as either:
§ Reassuring
§ Suspicious
§ Pathological
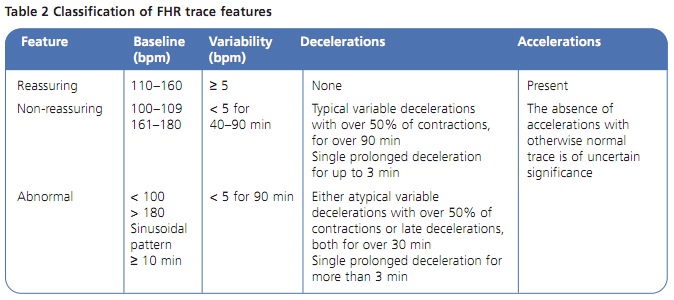
The overall impression is determined by how many of the CTG
features were either reassuring, non-reassuring or abnormal. The NICE
guideline below demonstrates how to decide which category a CTG falls into.
{kind=link}
{kind=link}
هیچ نظری موجود نیست:
ارسال یک نظر